Core Concepts for Grief-Sensitive Care
Current Approaches to Understanding Grief
Grief sensitivity involves leaning on accurate, up-to-date information related to current grief theory. In cultures that tend to avoid conversations about death and loss, knowledge about grief can stagnate.
This can leave both grieving people and those supporting them reliant on outdated models, assumptions, or myths that often fail to reflect the lived reality of grief.
Building grief-sensitive care involves a willingness to revisit what we think we know about grief and to replace inherited narratives with approaches that better reflect the complexity and variability of real grief experiences.
Moving Beyond the 5 Stages
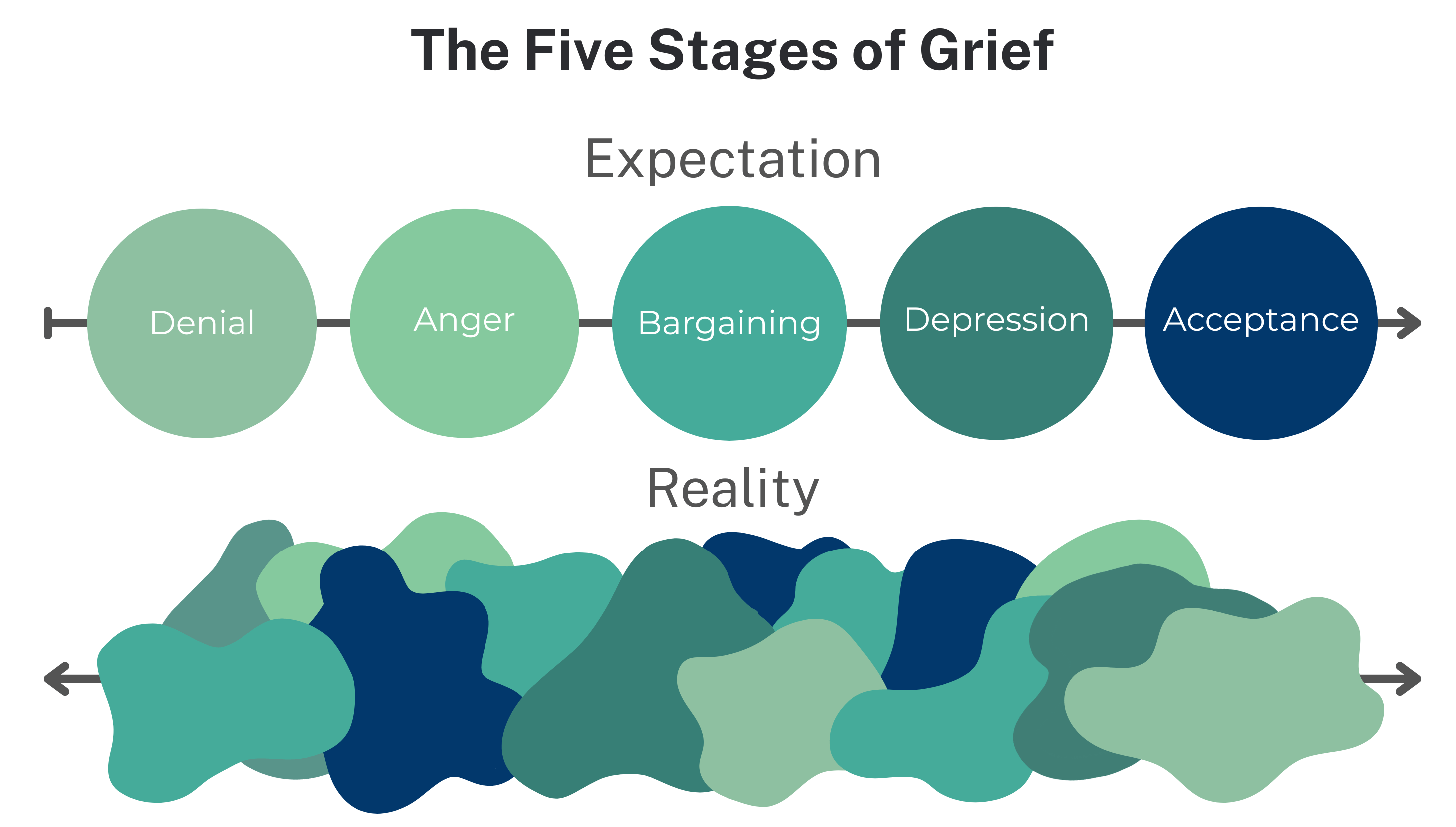
For many people, early education on grief theory was shaped by Elisabeth Kübler-Ross’s Five Stages of Grief, developed in 1969 to describe the experiences of people who were dying.
While Kübler-Ross’s work increased awareness and helped open conversations about death, the model was not intended to serve as a universal framework for bereavement.
Many grief professionals now view stage-based models as overly rigid. Another commonly cited concern is the lack of empirical evidence supporting stage-based models in bereavement, as these models were based on clinical observations of dying patients rather than systematic research with grieving individuals.
Expecting grief to unfold in neat, linear stages can create unrealistic expectations. When grief does not follow a prescribed sequence or timeframe, patients, supporters, or healthcare professionals may assume something is wrong, which can contribute to shame, isolation, and relational strain.
Stage-based frameworks may remain appealing because they offer a sense of order during distress. However, grief experiences are often non-linear, individualized, and shaped by context, meaning these models may not reflect the lived reality of grief for many people.
There are only two stages of grief: who you were before and who you are after.
Patients, families, or other care partners may reference the Five Stages of Grief. When someone asks “What stage am I in?”, this can be an opportunity to offer reassurance and gently reframe expectations.
Rather than dismissing the language someone is using, it can be helpful to validate the emotions they are describing. Feelings associated with denial, anger, or bargaining can be acknowledged as meaningful parts of the grief experience while also clarifying that grief does not unfold in fixed stages.
Grief-sensitive responses may include:
- “Grief does not follow set stages. It can look different for each person, and your experience is valid.”
- “There isn’t a checklist to move through. What you’re feeling can be a natural response to loss.”
- “Rather than stages, we often think of grief as something that changes over time. My role is to support you in a way that fits what you’re experiencing.”
By gently addressing misconceptions while validating the person’s experience, healthcare professionals can reduce pressure and help patients feel seen and supported in their individual grief experience.
There are several contemporary grief theories and frameworks that offer a more evidence-informed and realistic understanding of the grief experience.
The Dual Process Model of Coping with Bereavement
Developed by psychologists Margaret Stroebe and Henk Schut, the Dual Process Model of Coping with Bereavement (DPM) offers a dynamic, evidence-informed understanding of grief.
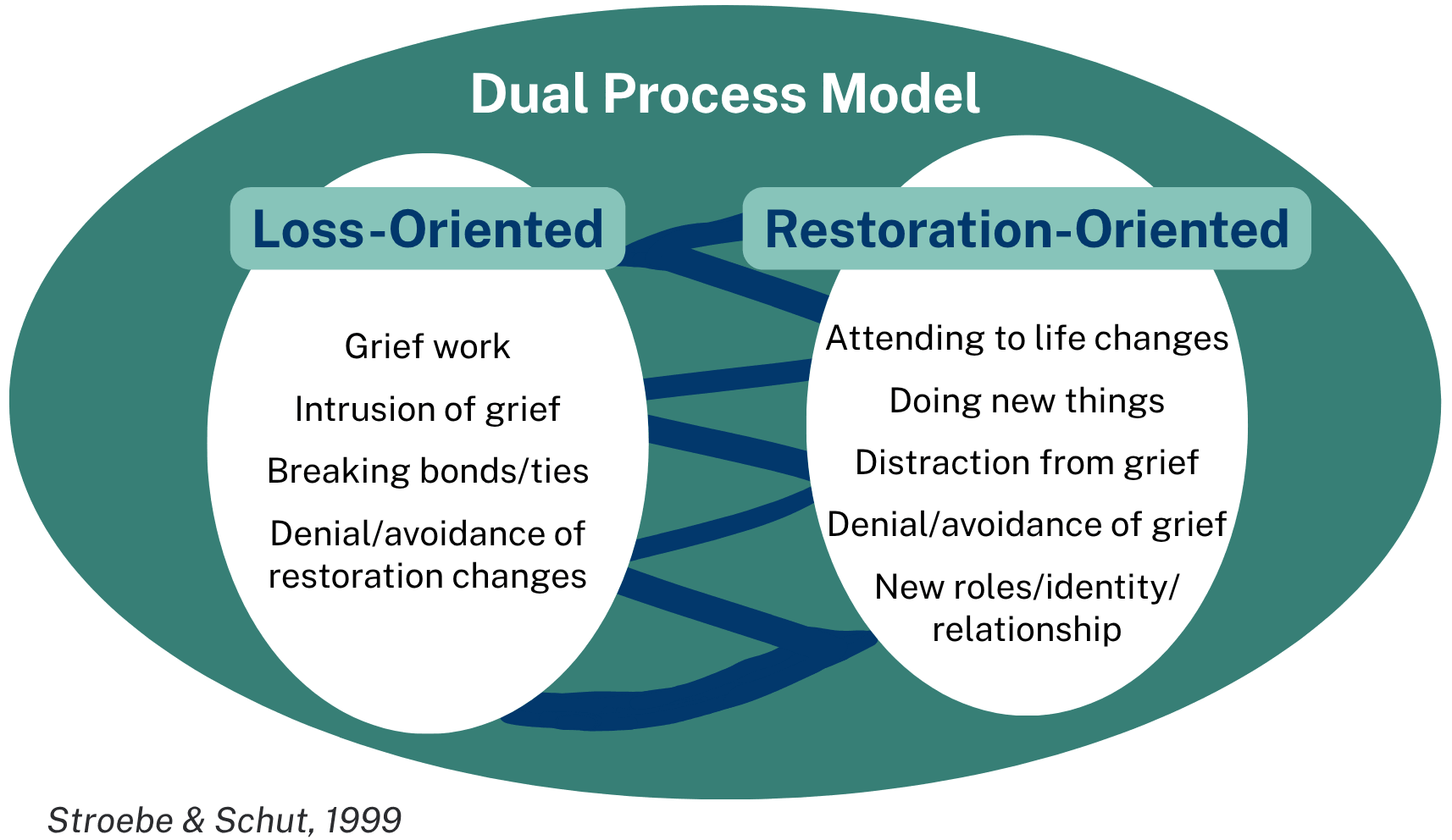
The model describes two types of coping responses that people may move between over time.
Loss-oriented coping focuses directly on the pain of the loss and may include emotional distress, yearning, revisiting memories, or difficulty with moving forward.
Restoration-oriented coping centers on adapting to life after the loss and may involve managing daily tasks, taking on new roles, reconnecting socially, or planning for the future.
People naturally shift between these two modes, a process known as oscillation. This back-and-forth is a normal part of grief and may be influenced by practical demands, such as caregiving or parenting, that require periods of day-to-day functioning alongside emotional processing.
Social and cultural factors can influence how people move between loss-oriented and restoration-oriented coping. For example, some family systems may emphasize “getting on with life,” which can discourage expressions of loss-oriented coping. Socialization may shape how grief is expressed, such as valuing stoicism while discouraging visible expressions of yearning or sadness.
This oscillation can help explain differences in coping between individuals. Two people grieving the same loss may appear to be on different paths depending on how they move between loss- and restoration-oriented coping. A person’s own grief responses may also differ across losses and relationships. While these differences can create tension within couples, families, or groups, recognizing them can reinforce that there is no single “right” way to grieve.
Dual Process Coping Across Healthcare Contexts
These examples illustrate how people naturally move between loss-oriented and restoration-oriented coping:
- A healthcare professional grieving a patient may express sadness and reflect on the care or the relationship, while also returning to work, supporting other patients, or engaging in team discussions or debriefings.
- A hospitalized patient after the death of a spouse may speak tearfully about their partner and shared memories, while also asking practical questions about discharge planning and living alone.
- A teen grieving a sibling may describe ongoing sadness or sleep difficulties during a routine visit, while also talking about reconnecting with friends or activities.
Recognizing this oscillation, in the context of social and cultural factors, can help healthcare professionals respond with flexibility and avoid misinterpreting grief responses.
Children’s Grief: Puddle-Jumping
Children often oscillate between loss and restoration activities more rapidly than adults, a pattern sometimes called "puddle-jumping," which is explained in this video, courtesy of Child Bereavement UK.
A child may appear sad or angry in one moment and engaged in play or laughter the next. This pattern is not avoidance or denial, but a developmentally common way of processing loss.
This variability is also reflected in Multidimensional Grief Theory, which describes how children’s grief often involves three primary bereavement-related challenges including separation distress (ongoing yearning and longing), existential/identity distress (feeling lost without the person), and circumstance-related distress (preoccupation with the way the person died).
Children may experience grief reactions in multiple domains at once or quickly shift from one reaction to another. They may also move from experiencing high levels of distress to playing or interacting with others as they normally would.
Scenario: A parent says, “My daughter cried a little when her grandfather died, but now she just wants to play. Is that normal?”
Grief-sensitive language you may use: “Yes, that can be very normal. Play is one way children make sense of their world. Children often move in and out of grief more quickly than adults, sometimes called ‘puddle-jumping.’ One moment they may feel sad, and the next they may want to play. That does not mean she is not grieving. Both sadness and play can be meaningful ways children cope.”
The Epigenetic Framework of Grief
Researchers Robert Neimeyer and Joanne Cacciatore describe an epigenetic framework of grief that emphasizes its non-linear and evolving nature. In this view, grief does not resolve once and for all. Instead, similar to biological processes that can be activated or altered by life events, grief may resurface and be reshaped across the lifespan.
New stressors, serious illness, or additional losses can reactivate earlier layers of grief. For healthcare professionals, this framework helps explain why a reaction may feel especially intense. The grief being expressed may reflect not only the current loss, but the layering of past and present grief experiences.
Recognizing grief as cumulative and developmental can support more empathetic and patient responses.
Prolonged Grief Disorder (PGD) was added to the DSM-5-TR in 2022. It refers to intense, persistent grief that can interfere with daily functioning and has previously been described as “complicated grief” or “persistent complex bereavement disorder.”
Its inclusion remains the subject of debate. Some view PGD as a way to better identify and support people experiencing severe, enduring grief, while others raise concerns about the risk of pathologizing a natural and highly variable grief experience.
Grief Persists: Tonkin’s Model
Many people do not experience grief as something they fully leave behind. Instead, grief may remain present while life gradually expands around it.
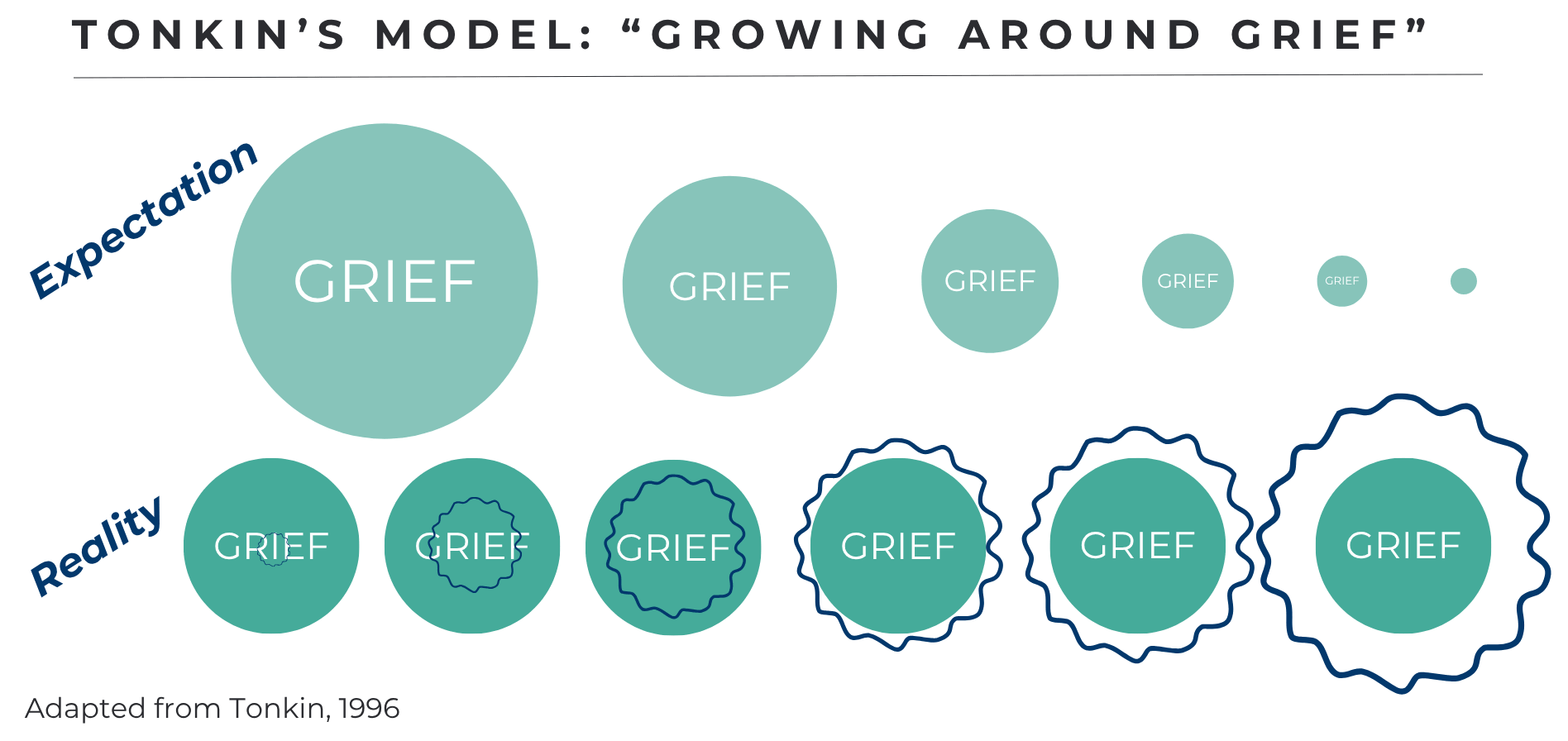
Lois Tonkin’s model describes this process by illustrating how grief remains even as a person’s capacity for meaning, connection, and daily life grows over time. This perspective can be supportive for grieving individuals and their supporters, particularly when there is pressure to “move on” or resolve grief. One does not “get over the loss” but rather continues to live with the loss.
Moving Beyond One Model of Grief
Regardless of the framework or model used, a central principle remains the same: grief is unique to each person and does not follow an orderly path with a clear endpoint.
Understanding grief as a dynamic and continuing experience, rather than a time-limited event, can support healthcare professionals in offering steadier, more compassionate care.